

 Home
Home Program
Program Exhibitors
Exhibitors My Meeting
My Meeting
 Virtual
Virtual Digital Posters
Digital Posters Case of Day
Case of Day


System Inefficiencies Lead to Duplicate CT Studies
Monday, Nov. 28, 2016
Acute trauma patients who receive imaging before being referred to a trauma center are likely to receive duplicate CT studies, leading to added radiation dose for patients and increased costs to the healthcare system, according to a study presented Sunday.

Ricarda M. Hinzpeter, MD
The study, presented by Ricarda Hinzpeter, MD, from the University Hospital Zurich in Zurich, Switzerland, retrospectively looked at all adult trauma patients transferred from other hospitals to a level-1 trauma center at University Hospital Zurich in 2014.
"CT is the modality of choice in the early imaging work-up of severely-injured patients," said Dr. Hinzpeter, who added that severely-injured patients are often transferred from regional hospitals to level-1 trauma centers and are re-scanned.
Dr. Hinzpeter and her colleagues analyzed repeated CT scans and categorized them according to the reasons for duplication, including inadequate CT image data transfer, poor image quality, repetition of head CT after head injury together with completion to whole-body CT (WBCT), and follow-up of injury known from previous CT.
They also calculated the cumulative radiation dose and costs associated with potentially preventable duplicative CT exams, which they defined as scans that were repeated because of inadequate image data transfer or poor image quality.
In this study 68 out of 298 patients whose conditions were not manageable in the referring hospital were transferred to the trauma center because of either severe head injury (n=45) or major body trauma (n=23). Seventeen other patients were transferred because they were being repatriated from a foreign country (n=14) or because there was no ICU capacity (n=3).
Of these 85 transferred patients, 74 (87.1 percent) had repeated CT scans. The reasons included:
- Inadequate CT image data transfer (n=29; 39.2 percent)
- Repetition of head CT with completion to WBCT (n=24; 32.4 percent)
- Follow-up of known injury (n=21; 28.4 percent).
None of the repeated CT studies were performed because of poor image quality.
Dr. Hinzpeter and her colleagues determined that the cumulative dose-length product of all of the repeated CT scans was 1,383 mSv or 18.7 mSv per patient, while patients who underwent potentially preventable repeat CT scans (those due to inadequate CT data transfer) received an overall additional effective radiation dose of 631 mSv, or 21.8 mSv per patient.
The additional costs associated with all of the repeated CT exams was $70,433, while the additional costs of potentially preventable CT exams was $38,961.
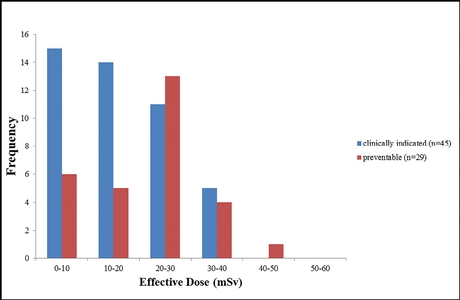
On a percentage basis, patients who underwent clinically indicated repeat CTs received lower effective radiation doses than patients who underwent potentially preventable CTs.
"A considerable number of transferred trauma patients undergo potentially preventable repeated CTs, adding radiation dose to the patients, and costs to the healthcare system," Dr. Hinzpeter concluded, adding that the main culprit was inadequate CT image data transfer.
"Future efforts should be made for improving and accelerating image data transfer, allowing for timely and complete availability of CT image data, even in the setting of acute trauma," she said.
Hatem Alkadhi, MD, of the University Hospital Zurich, who co-authored the study, pointed out that CT image data transfer of trauma patients to his hospital is performed either by manual transfer of CDs or via the internet. The problem is that in the case of acute trauma radiologists and clinicians want CT images made available as quickly as possible, even though the use of CDs is known to be hampered by incompatibilities with different computer and software systems.
And while the web-based transfer of images is feasible for patients who are being transferred in a non-trauma setting, it doesn't appear to be fast enough for some emergency situations.
So what's the solution? According to Dr. Alkadhi various initiatives for sharing radiologic images that are becoming available can easily solve the issue.
He noted that the use of a DICOM-email protocol has been proposed as a potential solution for fast and secure connections between hospitals causing minimal problems with existing firewall policies. And he added that another solution is streaming, which allows physicians at the trauma center to electronically access the images obtained in the regional hospital's emergency department, allowing trauma surgeons to review and evaluate CT images well ahead of patient arrival at the trauma center.